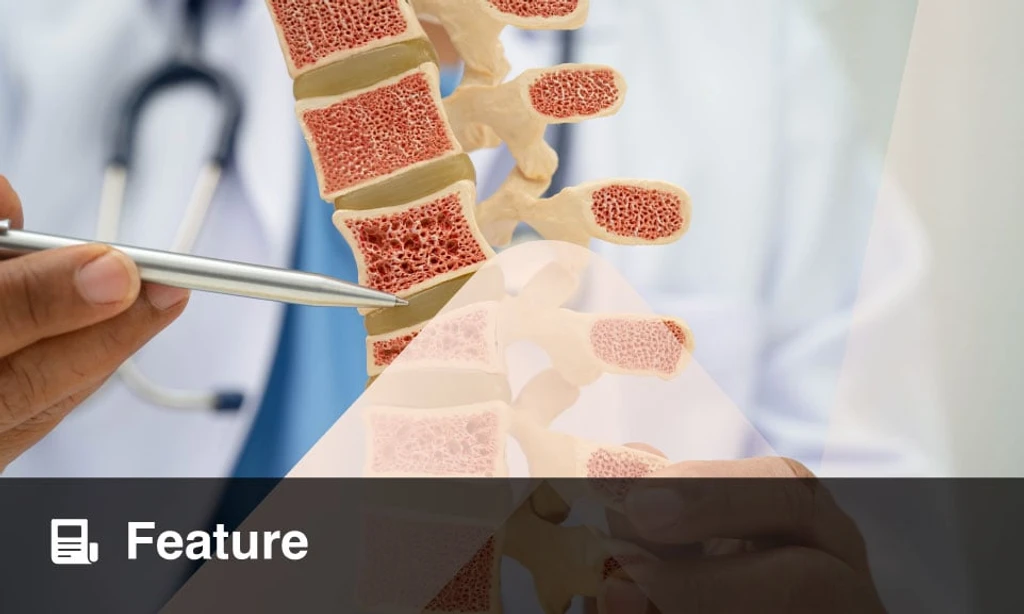
Type 2 diabetes (T2D) creates a silent skeletal crisis affecting millions. Chronic systemic inflammation and insulin resistance (IR) work synergistically to degrade bone architecture, often masking the threat behind normal or high bone mineral density (BMD).
This 'diabetic bone paradox' means fragility fractures occur despite seemingly healthy bone mass. The primary driver is a disrupted remodelling cycle where pro-inflammatory cytokines like TNF-α and IL-6 activate bone-resorbing osteoclasts while simultaneously inhibiting bone-forming osteoblasts.
Insulin is critical for anabolic bone formation. As IR progresses, osteoblast function plummets, collagen synthesis declines, and advanced glycation end products accumulate, making the collagen matrix brittle. Simultaneously, bone marrow stem cells shift toward fat production, further reducing bone quality.
Standard dual-energy X-ray absorptiometry (DXA) scans often fail to capture this damage. Clinicians are increasingly turning to the Trabecular Bone Score (TBS) for microarchitecture assessment and high-resolution peripheral quantitative CT (HR-pQCT) for 3D cortical and trabecular mapping. Biochemical markers reveal a globally suppressed bone turnover, distinct from typical postmenopausal osteoporosis.
Risk assessment tools like FRAXplus® now provide statistically significant adjustments for T2D patients who were previously underestimated. Therapeutic advances are focusing on the anabolic deficit, investigating GLP-1 receptor agonists for their potential bone-forming properties and exploring targeted sclerostin antibodies.
Postmenopausal women face a compounding risk as metabolic flexibility declines, linking ectopic fat accumulation to systemic frailty. For high-risk diabetics, integrating metabolic and skeletal risk stratification is no longer optional-it is essential to prevent devastating non-union fractures.