
A 42-year-old male with no significant medical history presented a diagnostic puzzle involving two months of fever, cough, breathlessness, and profound weight loss. Despite having no classic risk factors like HIV or diabetes, imaging revealed a startling multisystem infection.
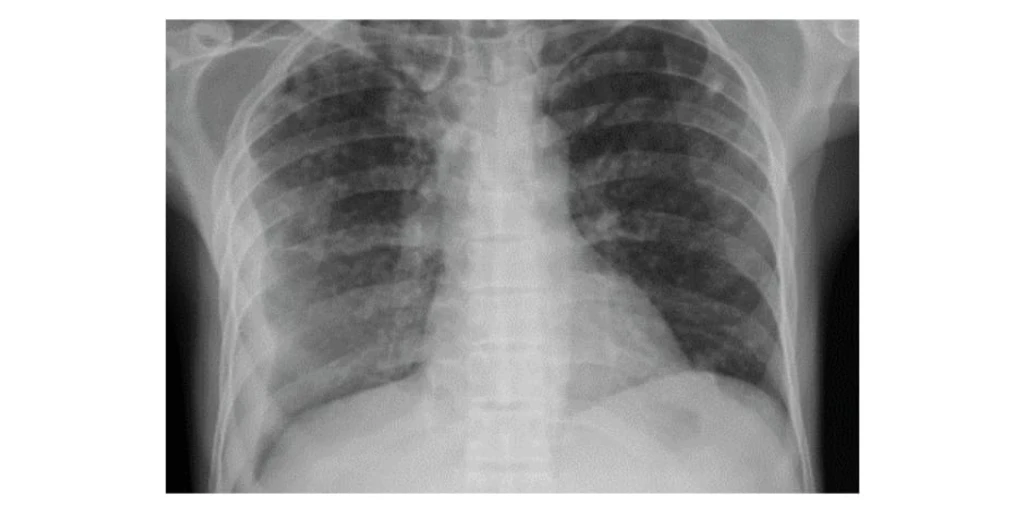
Examination showed the patient was frail, with reduced breath sounds and an enlarged liver and spleen. A chest radiograph confirmed bilateral nodular opacities and a right pleural effusion.
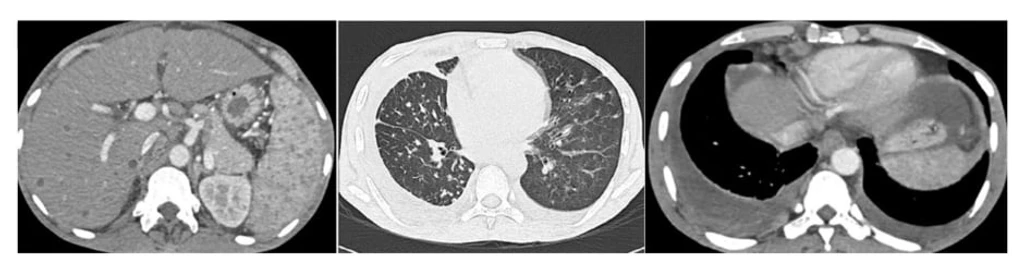
Advanced CT imaging of the thorax and abdomen revealed the full scope of the crisis: a right pleural effusion with a split pleura sign, bilateral pulmonary nodules showing a tree-in-bud pattern, necrotic lymph nodes, and hepatic microabscesses with splenic granulomas. The presentation strongly mimicked metastatic cancer.
To avoid risky invasive biopsies given his malnutrition, clinicians utilized rapid molecular testing. Cartridge-based nucleic acid amplification tests on both sputum and gastric aspirate confirmed Mycobacterium tuberculosis with no rifampicin resistance. The diagnosis of disseminated tuberculosis was established from multiple, easily accessible sites.
Antitubercular therapy was initiated, and surgery for a loculated pleural empyema was deemed too dangerous. The patient showed progressive clinical and radiological improvement over three months. Follow-up ultrasound confirmed the hepatic and splenic lesions were resolving.
This case emphasizes that disseminated TB must be on the differential for unexplained multisystem illness, even in immunocompetent adults. Early molecular confirmation from non-invasive samples can spare high-risk patients from unnecessary surgeries, leading to a favorable outcome.