
When a large language model (LLM) gives a cardiologist a poor answer, the briefing, or 'prompt', is often the problem. These tools are already handling discharge letters and guideline checks, yet adoption has outpaced proof of safety. A systematic review found only 5% of 519 studies used real patient data. LLMs can pass cardiology boards, but that reflects exam evidence, not bedside evidence.
A critical distinction exists between task-specific deep learning, validated in trials like the 22,641-patient AI-ECG screen, and generative LLMs. No LLM-based cardiology decision-support system has yet been CE-marked or FDA-cleared for autonomous clinical decision-making. The EU AI Act classifies medical AI as high-risk, mandating human oversight.
A randomized comparison showed blinded subspecialists preferred LLM-assisted assessments for complex cardiomyopathy cases, finding fewer clinically significant errors. But the cardiologist stayed in the loop. Another trial found physicians using an LLM scored no better than those using conventional resources, even though the model alone outscored both. Worse, a confidently wrong LLM can drag clinicians down with it.
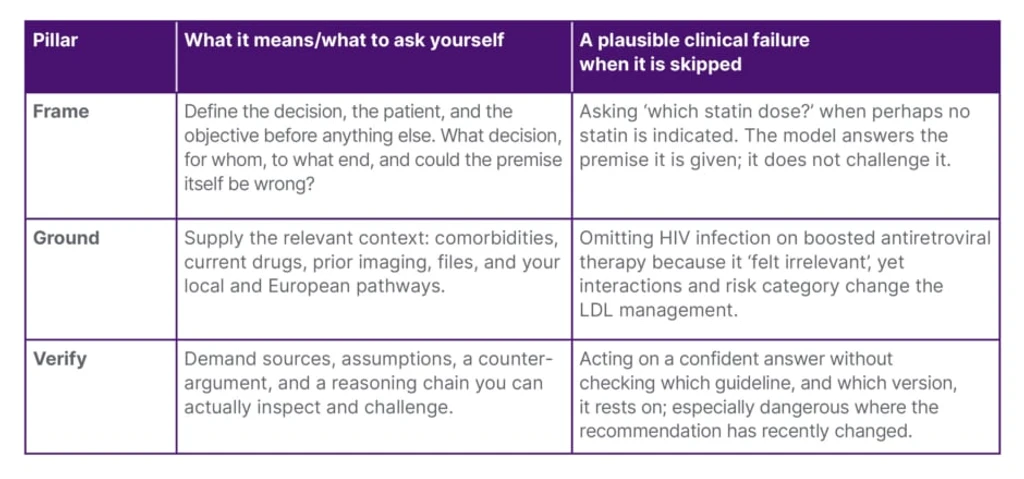
The conceptual shift of 2026 moves from polishing wording to engineering context. In 600 evaluations of complex coronary cases, supplying European guidelines in the prompt raised the model's score from 6.9/10 to 7.7/10. The briefing has three pillars: framing the question, grounding it in patient context, and demanding a verifiable reasoning chain.
The honest limitation is that almost all studies are scenario-based, not bedside. A pragmatic randomized trial embedding an LLM in real interventional workflows has never been done. Until then, the discipline is to treat the model as a co-pilot, learning to brief it with frame, ground, and verify. The model will change; the skill of asking the right question endures.